



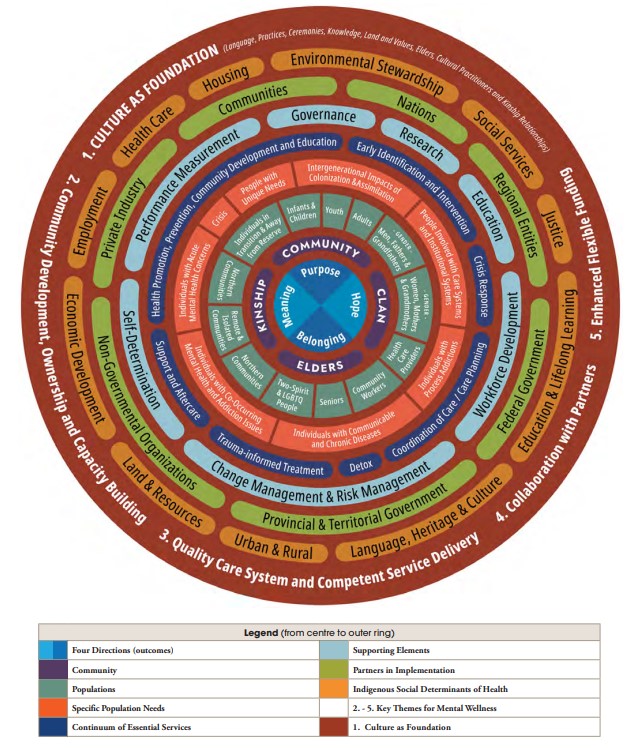
In this image, we see a river flowing and its waters are clear with big rocks. Along this river, two individuals prepare to embark on a journey in their kayaks. The river represents the path of life, and the rocks symbolize the challenges indigenous children experience, such as historical trauma, mental health issues, ACEs, and more.
The first individual is equipped with sleep, enough nutrition, and emotional and social support at home. He wears a t-shirt with the word, “hope,” symbolizing optimism he has cultivated in his life. These protective factors act as his paddle, helping him steer around the rocks, and help navigate the turbulent waters ahead. The second individual, wearing a red top, has learned his traditional ways, his language, and culture. These protective factors are also important to healing and understanding the community and environment. The outdoor environment, rich with natural beauty, reinforces the importance of connecting with nature and their indigenous roots.
As they paddle downstream, they learn to move like water, flowing around obstacles rather than being stopped by them. The combination of protective and cultural factors helps them navigate life’s adversities and allows them to be one with water—adaptable, renewed, and healthy. Together, they demonstrate that with the right support and connection to their community, nature, and self, they can overcome any challenges the river of life presents.

Two Feathers Native American Family Services (NAFS) is a light of hope and healing in Humboldt County, California. As a national leader in advancing Native mental health, Two Feathers NAFS employs innovative approaches that emphasize community building, honoring cultural identity, values, and traditions. Their mission is to address mental health challenges in geographically isolated and economically disadvantaged regions, and they envision a world filled with love and balance.1
They are dedicated to helping Native youth and their families achieve their full potential through culturally tailored mental health programs.
Chekws Counseling & Family Services is one of their cornerstone programs. It offers individual counseling, youth leadership programs, equine therapy, cultural programming, and intensive case management.1 These services are designed to strengthen family attachment, improve crisis management, reduce risk–taking behaviors, and enhance life skills. The program is built on a culturally responsive, trauma-informed framework that prioritizes access to cultural knowledge and addresses systemic inequities.1
The A.C.O.R.N. Youth Wellness Program focuses on teaching cultural values and their application to physical, mental, spiritual, and cultural aspects of daily life. The goal is to decrease trauma symptoms, improve relationships, and create a sense of hope through activities like inter–tribal drumming, song and dance, storytelling, art, basket–weaving, dress making, and trips to cultural events.1
Two Feathers NAFS is a trailblazer of how culturally tailored mental health services create profound and positive changes in Indigenous communities. Their dedication to honoring traditions while addressing modern challenges sets a powerful example for others to follow.
NIHB visited Two Feathers Native American Family Services to learn more about their programs. Two Feathers NAFS is a national leader in Native mental health advancement through a blend of innovative approaches that center community building and cultural affirmation to address long standing mental health challenges in Two Feathers’ geographically isolated and economically challenged region.
Here are photos from our site visit:






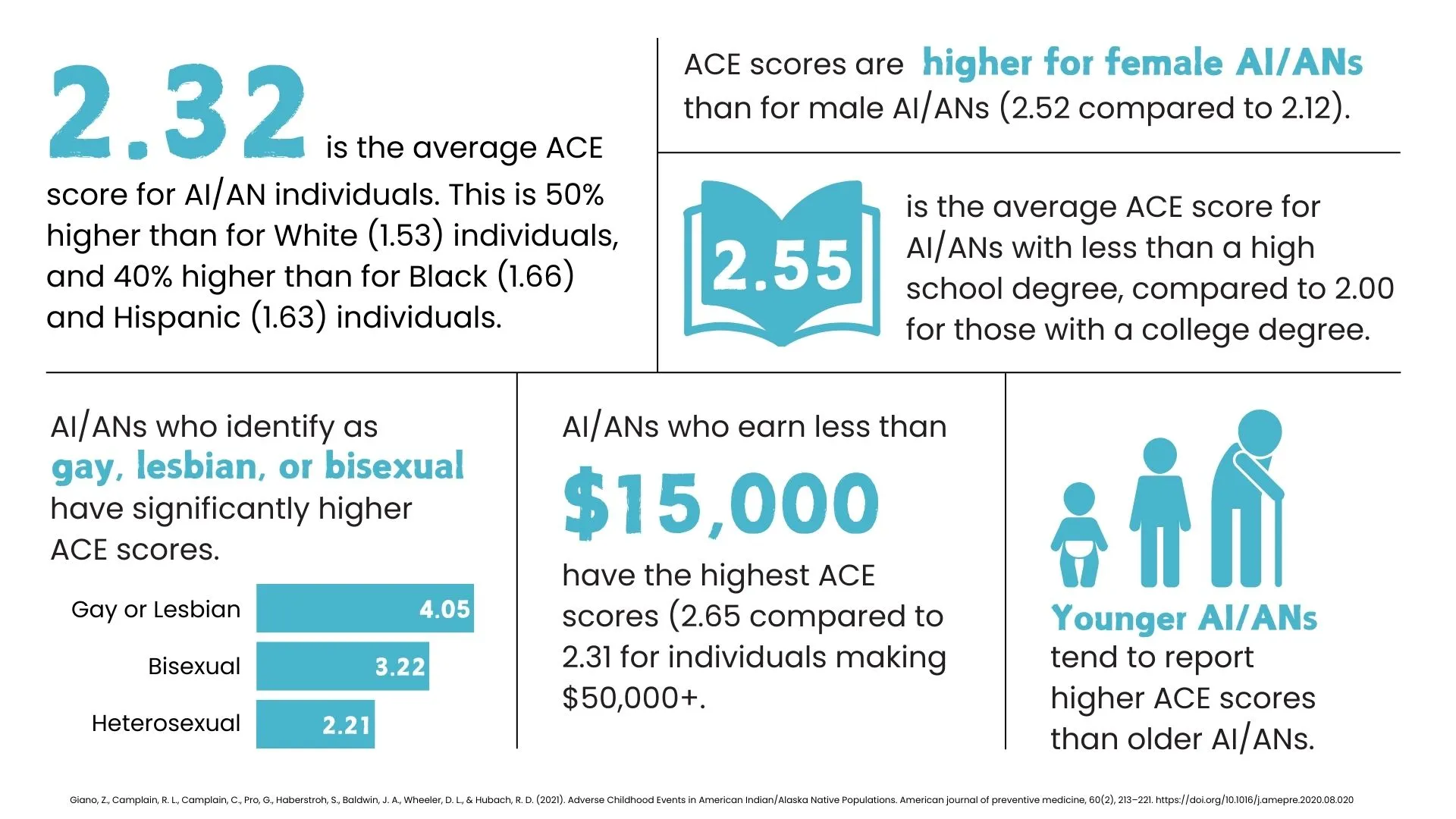
Radford et al., (2021) explored the impact of ACEs on the health and wellbeing of Indigenous populations in North America. They found that Indigenous peoples have higher ACE scores compared to non–Indigenous groups, which are linked to depression, substance use, and chronic pain.1 However, current research often overlooks the historical and social contexts of Indigenous communities, such as the effects of colonialism and boarding school experiences.1 While the ACE model helps explain health disparities, it doesn’t capture the full complexity of Indigenous experiences. Other studies have shown that spiritual activities and a strong sense of cultural identity are associated with positive mental health outcomes despite having ACEs.1

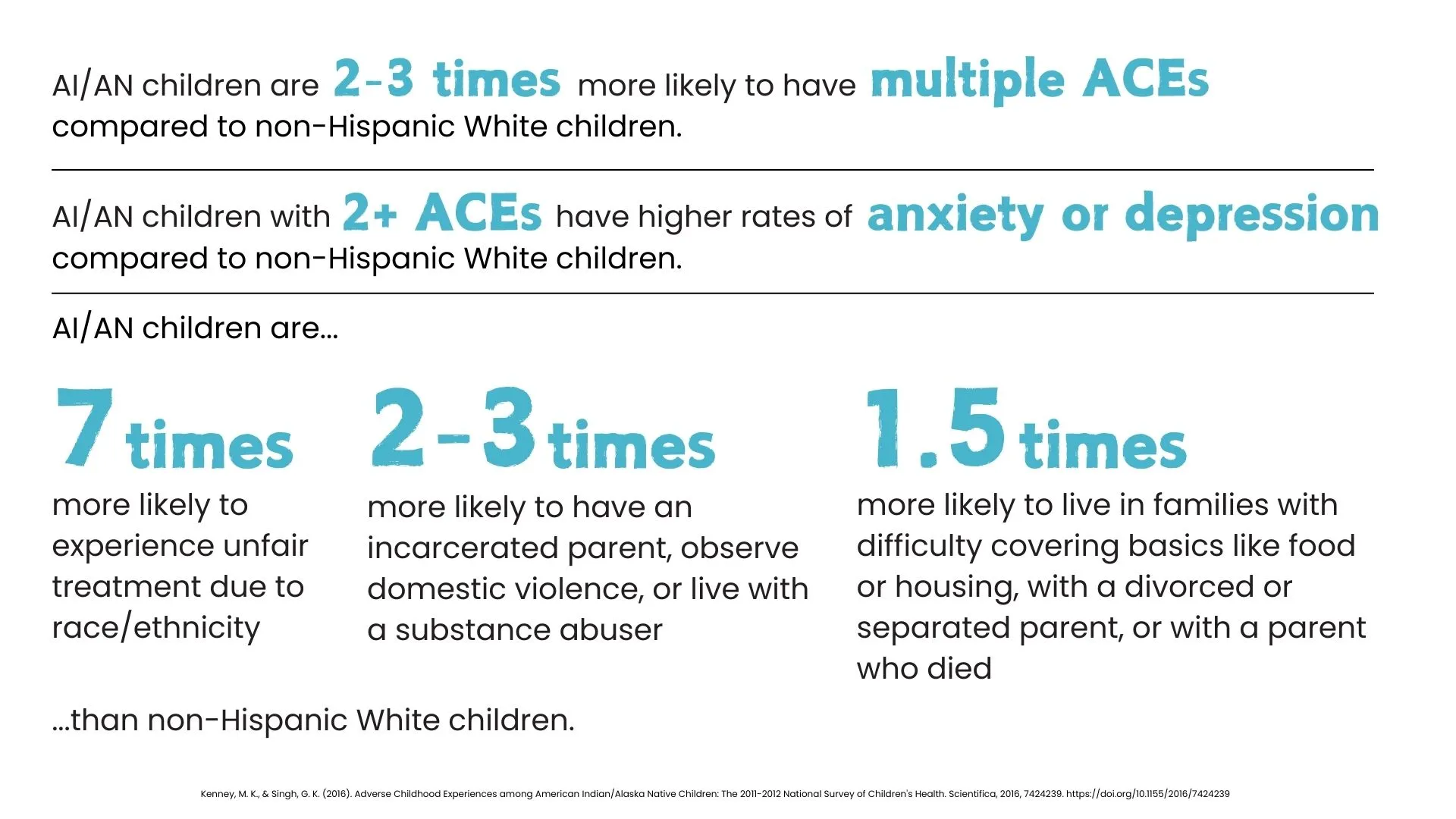
Edwards et al., (2023) found that a strong connection to Indigenous culture serves as a protective factor against ACEs.2 Indigenous children often experience multiple ACEs with an average of four ACEs in just six months.3 They also found that caregivers deeply rooted in their culture show a weaker correlation between their own ACEs and those of their children.2 This suggests that cultural identity, traditional practices, and values can help break cycles of trauma, although social support alone is less effective and more complex. Broader family and community dynamics may offer additional protection against ACEs.2
Rides At The Door & Shaw, (2023) emphasize the need for Indigenous communities to address historical and intergenerational trauma to heal effectively.3 They propose the Indigenous Wellness Pyramid Framework, which integrates individual, family, community, and societal levels. This framework respects Indigenous sovereignty and decision-making, and it considers Indigenous healing practices as legitimate as Western medicine.3 They believe the goal is not just to extend life expectancy but to make sure that elders contribute to intergenerational healing and community sovereignty.4 This long–term process requires community–wider mobilization and ongoing efforts to restore balance and wellness among Indigenous communities.3
The First Nations Mental Wellness Continuum (FNMWC) is a framework designed for Indigenous peoples, grounded in culture, language, and traditional knowledge.4 It promotes holistic well–being by addressing mental and substance use challenges, while providing a roadmap for communities to enhance their mental wellness programs through collaboration and culturally appropriate health services tailored to their unique needs.4
The Historical Oppression, Resilience, and Transcendence Framework by Burnette and Figley (2017) offers a deeper understanding of how Indigenous communities demonstrate resilience in overcoming adversity.5 This framework focuses on the interconnectedness of mental, emotional, physical, and spiritual health and promotes a holistic approach to well–being. It also focuses on the development of protective factors, such as community support and cultural practices, which improve the capacity to cope with ACEs.5
The Indigenous Wellness Framework, created by the Thunderbird Partnership Foundation, focuses on cultural interventions delivered by knowledgeable Cultural Practitioners or Elders that impact the whole person—spirit, heart, mind, and body.6 The holistic approach creates a deep connection to one’s culture and promotes overall wellness.

The Substance Abuse and Mental Health Services Administration’s (SAMHSAs) Strategic Prevention Framework (SPF) offers a valuable approach for addressing high ACE scores. It provides a structured method for tackling substance misuse through five steps: Assessment, Capacity, Planning, Implementation, and Evaluation, while being guided by cultural competence and sustainability principles.7 However, this framework shouldn’t be used alone. Integrating it with an Indigenous framework or perspective can create a strategy that address both immediate and long-term needs that create well-being in Indigenous communities.

CDC’s Comprehensive Approach to Preventing ACEs uses multiple strategies derived from the best available evidence. These strategies focus on primary prevention but also include strategies to reduce long–term consequences of ACEs.8 The figure below highlights these areas. This approach may not incorporate the unique, cultural, historical and social contexts of Indigenous communities, especially the limited resources and poor infrastructure in remote and economically disadvantage areas of Indian Country. Without addressing these barriers, the strategies suggested may not reach those who need them most.
To further support these efforts, connecting Native youth to caring adults and activities, such as mentoring and after–school programs are beneficial. Having Indigenous approaches that involve the community, culture, and trauma–informed care can significantly improve health outcomes for those with a history of ACEs.
 |  |  |
| Module 1 Lesson 1: ACEs, Brain Development, and Toxic Stress 10 | Module 1 Lesson 2: The ACE Study 11 | Module 2 Lesson 1: ACEs 12 |